
What should an obstetrician do when nuchal cord is reported on an ultrasound late in pregnancy?
Google ‘nuchal cord’ at your own risk. You will be taken to many informative sites, but you will also be exposed to the internet pregnancy forum and many more anti-medical, often biased and potentially misleading opinions. But are we being equally biased in our response to some of the lay (and medical) opinions expressed on the web? Have we allowed the nuchal cord to become a noose around our necks (…sorry) thereby over reacting to a natural fetal event or have we ignored a serious issue?
Hippocrates described nuchal and chest coiling of the umbilical cord as: ‘One of the great dangers of the eighth month’. He also stated that persistence of the nuchal cord ‘will cause suffering to the mother and either perish or born difficulties to the fetus’.1 More recently, in 1750, William Smellie described a stillborn with four nuchal loops2; and in 1769, Andrew Bell published a drawing in the Encyclopedia Britannica depicting a fetal death with one nuchal cord, a body loop and a true knot.3
In 2010, then, what are the important questions we must ask and answer regarding nuchal cord? I propose the following questions:
- Does nuchal cord predispose to significant, persistent neonatal morbidity and perinatal mortality?
- Should the presence of nuchal cord be examined for when performing third trimester ultrasound and should its presence be reported? Leading finally to the most challenging question of all:
- Does antenatally identified nuchal cord require obstetric intervention?
Background
The definition of nuchal cord (NC) – ’the condition in which the umbilical cord is wound at least once around the neck of the fetus’ – is attributed to Dr J Selwyn Crawford, a British obstetric anaesthetist, in 1962.4 In studies of 468 babies with nuchal cord, he remarks that there is an increased liability to neonatal depression.5 Prior to this, Shui’s study of 1000 consecutive deliveries in 1957 did not find any correlation with perinatal mortality and the presence of a single NC.6 The question of the significance of NC has persisted since that time.
In 1988, Giacomello described two types of NC, in relationship to breech presentation7:
- Type A – nuchal loop that encircles the neck in a freely sliding pattern.
- Type B – nuchal loop that encircles the neck in a locked pattern.

Reprinted with permission from TheFetus.net, ultrasound diagnosis of quintuple nuchal cord entanglement and fetal stress, Silva et al.
The significance of this differentiation is that type B cord loops may result in true knots in the cord, should the fetal body slip through the ‘noose’. Collins observed that the type B pattern occurred in one in 50 births and that operative delivery and stillbirth were more common with this type of NC.8
Many others further differentiate NC presentations as loose versus tight and single versus multiple in an attempt to potentially identify and record the ‘pathological’ NC. A loose NC can easily be uncoiled before delivery of the fetal trunk. The NC is considered tight when it requires clamping and cutting before delivery of the trunk.9
Natural history
NC is found in 20 per cent of babies at delivery (range 15 to 34 per cent).4,5,6,10,11 The majority are single loops, with double loops found in 1.7 to 3.8 per cent and three or more loops in 0.2 to 0.3 per cent.6,12,13 Twenty-five percent of cord loops are tight, though this figure is higher for multiple loops (60 per cent).9
Prospective studies through pregnancy using ultrasound indicate that NC can resolve and recur throughout pregnancy. However, the later they are noted in pregnancy, the more likely they are to persist to term.12,14,15 In studies by Lal14, Larson12 and Clapp15 the incidence of NC was six per cent at 20 weeks; 7.5 per cent to 15 per cent at 30 weeks; 25 per cent at 36 to 38 weeks; and 28 to 37 per cent at birth. Lal found that of those fetuses with NC at 36 to 38 weeks, 85 per cent persisted until delivery. Clapp found that 60 per cent of fetuses had a NC identified at some time during pregnancy, with only 25 per cent persisting for more than four weeks.
The sensitivity of colour Doppler ultrasound in detecting NC has been reported to range from 38 per cent to 96 per cent and the positive predictive value between 30 to 82 per cent.16,17,18 ultrasound can distinguish between single and multiple nuchal loops, but cannot reliably identify tight NC.18
Outcomes
Somewhat disparate findings regarding obstetric/antenatal associations and outcomes of NC have been reported over the past 40 years. The presence of NC at delivery is not associated with increased perinatal mortality, but has been reported by some to be associated with increased incidence of fetal CTG abnormalities (consistent); meconium stained liquor (inconsistent); low APGAR scores; umbilical artery acidosis (inconsistent); operative delivery in nulliparas; IuGR (inconsistent); neonatal resuscitation; admission to NICU; and neonatal anaemia and cerebral palsy, with varying degrees of significance.4-6,9-11,15,17,19,20-28 The overall conclusion of these studies is that NC identified at delivery is not associated with significant, persistent adverse perinatal outcomes. The presence of NC on ultrasound does not appear to be associated with increased perinatal mortality15,19,21, however, studies to date have not had the power to address this question, as the approximate rate of NC associated stillbirth would be approximately 0.2 to 0.27 per 1000 births or one in 3700 to 5000 births (excluding true knots and other ‘cord accidents’).3
In a prospective blinded study, examining 84 fetuses through pregnancy and delivery, Clapp found no significant difference between outcomes in the NC group and controls, other than an increased incidence of fetal heart rate abnormalities in labour in the NC group.15 Interestingly, persistence of antenatal NC for later than four weeks was associated with a 75 per cent incidence of asymmetric growth restriction, and though CTG monitoring was normal, these babies also demonstrated some cerebral blood flow distribution. In a prior retrospective study, Clapp made a similar observation regarding persistence of antenatal NC and mild growth restriction. In that study, it was found that multiple nuchal loops, tight cord at delivery, symptomatic NC in labour (fetal heart rate abnormalities with or without meconium), and antenatal persistence of NC, were significantly associated with subclinical deficits in neurodevelopmental scores at one year of age. These differences were not seen in babies with no NC or incidental NC (uncomplicated labour and delivery). Clapp’s conclusion was:
‘There may be a continuum in outcome following NC ranging from an entirely normal short and long-term outcome through a variety of short-term morbidities and minor subclinical deficits in development to the extremes of intrauterine demise or spastic quadriplegia.’20
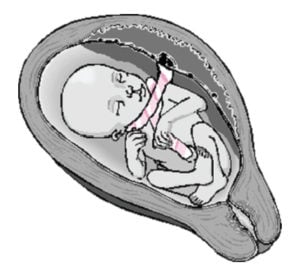
The pathology of NC may be related to acute, chronic or intermittent cord compression, resulting in fetal hypoxia, biochemical derangements and circulatory shunting. It is postulated that length of cord; position of placenta and cord insertion relative to the fetus; number, type and tightness of nuchal loops; coiling and relative thinness of cord; presence of cord knots or truncal loops; and abnormal fetal movements may all interact to predispose to pathological cord compression and adverse outcome.3,20

Reprinted with permission from obgyn.net: Nuchal Cord by: Mario Ernesto Libardi.
Management of the antenatally identified nuchal cord
Is there evidence to suggest that ultrasound assessment for the presence of NC should be part of routine ultrasound scanning or antenatal care? No. The presence of NC alone is unhelpful in predicting the fetus at risk of significant cord compression and ultrasound (at this time) has been unable to identify additional markers of concern other than multiple nuchal loops. Therefore, routine assessment for NC prior to delivery is of no benefit.
However, it is common practice for sonographers to note the presence/absence of NC when imaging the breech fetus prior to external cephalic version (ECV) or planned vaginal delivery. NC is considered by some to be a relative contraindication for ECV, though the evidence for this is lacking.30 Likewise, if NC is identified when imaging for other indications in the third trimester, it is not uncommon for this to be noted by the sonographer and the reporting radiologist.
The dilemma then, is what to tell the mother and whether further monitoring or other management is required. It is reasonable care to inform your patient that the ultrasound has identified a NC and to discuss the limitations of ultrasound, the common occurrence of NC and the chance that it may resolve before delivery. Advise the woman to monitor fetal movements and report unusual increases and decreases in fetal activity.
Increased monitoring for simple NC remote from term does not appear to be indicated.21
Induction of labour for single NC is not indicated in the absence of other indications. Caesarean section is not indicated in the absence of fetal concerns or compromise.
The management of multiple NC is less certain, but again, vaginal delivery at term is not contraindicated. Fetal heart rate monitoring in early labour is suggested. There is no clear indication for elective caesarean section, but this is at the discretion of the treating obstetrician and the mother, given the evidence in some studies of greater risk of meconium, abnormal fetal heart rate pattern, operative vaginal delivery and mild umbilical artery acidosis at birth with multiple NC.29
Further studies are required to identify the antenatal factors associated with NC that increase the likelihood of significant adverse outcome and what obstetric interventions (if any) will prevent adverse outcome.
References
- Hippocrates: De Octimestri Partu.
- Smellie W. A Treatise on the Theory and Practice of Midwifery. Volume 1, 1752.
- Collins JH. umbilical Cord Accidents 2010. Available from: www. preginst.com/ .
- Crawford JS. Cord round the neck. Incidence and sequelae. Acta
paediat. 1962; 51:594. - Crawford JS. unpublished data referenced in comments in BMJ; 17 October 1964.
- Shui KP, Eastman NJ. Coiling of the umbilical cord around the fetal neck. Br J Obstet Gynaecol. 1957;64:227-9.
- Giacomello F. ultrasound determination of nuchal cord breech presentation. Am J Obstet Gynecol. 1988; 159:531-2.
- Collins JH. Nuchal cord type A and type B. Am J Obstet Gynecol. 1997; 177(1): 94.
- Shrestha NS. Nuchal cord and perinatal outcome. Kathmandu
university Medical Journal 2007; 5 (3):360-363. - Ghosh GS. Nuchal cord in post-term pregnancy – relationship to suspected intrapartum fetal distress indicating operative intervention. J Perinat Med. 2008;36(2):142-4.
- Sheiner E, et al. Nuchal cord is not associated with adverse perinatal outcome. Arch Gynecol Obstet. 2006; 274: 81-83.
- Larson JD, Rayburn WF, Harlan VL. Nuchal cord entanglements and gestational age. Am J Perinatol. 1997; 14(9):555-7.
- Carey JC, Rayburn WF. Nuchal cord encirclements and birth weight. J Reprod Med. 2003; 48(6):460-2.
- Lal N, et al. Does the nuchal cord persist? An ultrasound and color-Doppler-based prospective study. J Obstet Gynaecol Res. 2008; 34(3):314-7.
- Clapp JF. The natural history of nuchal cords. Am J Obstet Gynecol. 2003; 189:488-93.
- Aksoy u. Prenatal color Doppler sonographic evaluation of nuchal encirclement by the umbilical cord. J Clin ultrasound. 2003;
31(9):473-7. - Peregrine E, et al. ultrasound detection of nuchal cord prior to
labor induction and the risk of Cesarean section. ultrasound Obstet Gynecol. 2005; 25(2):160-4. - Qin Y, et al. Color ultrasonography: a useful technique in the identification of nuchal cord during labor. ultrasound Obstet Gynecol. 2000 May; 15(5):413-7.
- 19. Assimakopoulos E, et al. Nuchal cord detected by ultrasound at term is associated with mode of delivery and perinatal outcome. Eur J
Obstet Gynecol Reprod Biol. 2005; 123(2):188-92. - Clapp JF, et al. Nuchal cord and neurodevelopmental performance at one year. Am J Obstet Gynecol. 2003; 189(2):488-93.
- González-Quintero VH, et al. Outcomes of pregnancies with sonographically detected nuchal cords remote from delivery. J
ultrasound Med. 2004; 23(1):43-7. - Jauniaux E. Perinatal features of pregnancies complicated by nuchal cord. Am J Perinatol. 1995; 12(4):255-8.
- Martin GC. Acidosis in newborns with nuchal cords and normal Apgar scores. J Perinatol. 2005; 25(3):162-5.
- Mastrobattista JM, et al. Effects of nuchal cord on birthweight and immediate neonatal outcomes. Am J Perinatol. 2005; 22(2):83-5.
- Miser WF. Outcome of infants born with nuchal cords. Journal of
Family Practice 1992. - Nelson KB, et al. Potentially asphyxiating conditions and spastic cerebral palsy in infants of normal birth weight. Am J Obstet Gynecol. 1998; 179(2):507-13.
Contact O&G Magazine for a full list of references for this article.


Leave a Reply