Women’s health has been a passion for me ever since I graduated as a doctor from the Fiji School of Medicine in 1978. After an internship and a stint in community health, I joined the obstetrics and gynaecology department at the Colonial War Memorial Hospital in Suva. I was fortunate to be a student of Dr Mary Schramm, an iconic figure in women’s health in Fiji. Dr Schramm was passionate about her work, a great teacher and an excellent role model. She emphasised the basics in understanding clinical medicine and was compassionate and dedicated to her work in Fiji.
In 1986, I was fortunate enough to receive a WHO fellowship to go to Wellington for a year to do the Diploma in obstetrics. On my return, I worked in Lautoka until the military coup in 1987. I was committed to becoming a specialist in obstetrics and gynaecology. This led me to National Women’s Hospital in Auckland and then, in 1990, to the Royal Hospital for Women in Sydney.
Life was not easy for overseas-trained doctors. While my traineeship was being organised, I worked as a research fellow in menopause under the mentorship of Drs Barry Wren, John Eden and Michael Webster. After completing my membership exams in 1994, I continued at the Royal as a senior registrar and, on obtaining Fellowship, joined the academic unit with Prof Michael Bennett, Drs Leo Leader and Steve Horowitz, where I stayed until 2011.
In 2011 my husband, Rajat Gyaneshwar, and I started a charitable trust to run the Viseisei Sai Health Centre (VSHC) in Fiji and we continue to work here. My strong background in clinical obstetrics and gynaecology, research and academic interests is being put to good effect in my new roles. I still work as an academic at the Fiji National University and Lautoka Hospital. However, my main focus now is to empower women and girls about their reproductive health as their basic human right. The political uncertainties in Fiji since 1987 have led to a health system that has become progressively less effective, owing to loss of human resources to other countries and a health budget that is stretched to provide essential services.
In spite of many decades of concerted effort by the Ministry of Health and its development partners – such as the UNFPA, Secretariat of the Pacific Community (SPC) and the World Health Organization (WHO) – the health indicators suggest marginal or no improvement. The contraceptive uptake rate (<40 per cent) is low with consequent high rates of unplanned pregnancies, particularly in rural areas, high teen pregnancy (ten per cent of all deliveries), sexually transmitted infections and female cancers.1 All these factors contribute significantly to the disempowerment of women and girls, which is a major reason for their vulnerability to the discrimination and violence perpetrated against them.
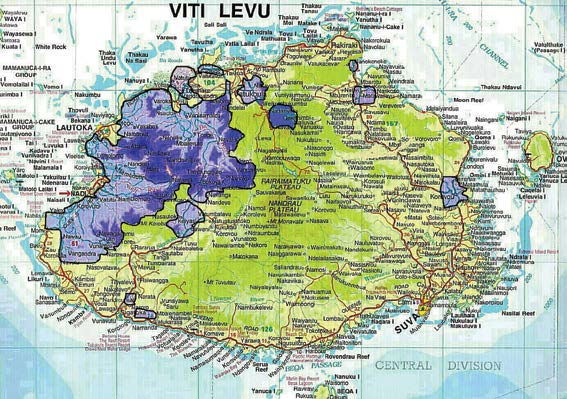
Areas covered in Viti Levu, Fiji (in purple) under the reproductive health outreach
education and clinics project.
Mortality associated with non-communicable diseases (NCDs) remains high at 82 per cent of all adult deaths, many of which are premature. Overall average life expectancy of 64 for males and 69 for females is low and days lost from work owing to illness high.2 The country’s Ministry of Health conducted a WHO STEP survey3 in 2002, repeated in 2011, which reported the common NCDs in Fiji: hypertension with prevalence rates of 24.2 per cent in 2002 increased to 31 per cent in 2011; diabetes at 19.6 per cent in 2002 increased to 29.6 per cent in 2011; and obesity at 58.5 per cent in 2002 increased to 66.9 per cent in 2011. Adult motility in Fiji is three times higher than in Australia and New Zealand. These worsening NCD rates are alarming, but can be prevented and reduced by modifying lifestyle factors, as shown in other countries.4
In 2008, the United Nations Development Project (UNDP) Pacific Centre reported that the basic needs poverty has increased and their economic modelling predicts a worsening trend in rural households in Fiji. Using this it is estimated that 50 per cent of households in rural communities will experience basic needs poverty.5 Poverty is exacerbated by early deaths and disability caused by NCDs as well as lack of employment opportunities and lost educational opportunities owing to unplanned pregnancies, particularly in teenagers. Data from VSHC project have shown, in rural women, the higher the number of children the greater the number of unplanned pregnancies. This is a manifestation of their disempowerment, owing to the lack of adequate information and awareness about contraception. Violence against women is high, with 64 per cent of women in Fiji reporting they have been in an intimate relationship having experienced violence in their lifetime.6 In this context, I have a strong commitment to the education of women and girls about their reproductive health as well as the Viseisei community in wellness and NCD prevention.

The author talks to schoolgirls as part of the outreach project.
I have just completed a project funded by the European Union, under its human owing to the lack of adequate information and awareness about contraception. Violence against women is high, with 64 per cent of women in Fiji reporting they have been in an intimate relationship having experienced violence in their lifetime.7 In this context, I have a strong commitment to the education of women and girls about their reproductive health as well as the Viseisei community in wellness and NCD prevention.
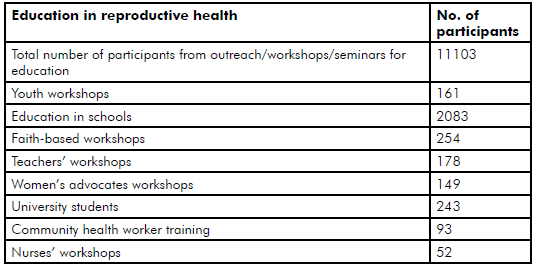
Table 1. Educational activities: February 2013 to December 2014.
I have just completed a project funded by the European Union, under its human rights instrument 8, in which our team went out to remote villages and settlements to educate, provide counselling and clinical services in reproductive health. We have conducted a study to identify gaps in knowledge, attitudes, practice and barriers to look after their reproductive health, especially in regards to safe sex and cervical cancer screening.
More than 70 per cent of a total of 1505 rural women surveyed in a baseline survey conducted by the VSHC had no knowledge of reproductive health issues such as cervical cancer and its prevention. This project has been about empowering women to exercise their health rights by providing them with information and outreach clinical services in family planning and contraceptive use.
Through the project, the VSHC has provided rural women and girls with access to information on reproductive health, conducted 161 outreach clinics and provided educational and clinical services to more than 11 000 rural women and girls. Apart from clinical services, counselling and educational workshops, the centre has also conducted awareness campaigns on reproductive health with various groups, including men and boys. Reproductive health is a human right denied to many women and girls because of gender inequality, lack of information and their ability to make informed choices about themselves. This leads to serious consequences for a woman, her ability to realise her full potential and participate in society fully.

Consulting in the privacy of the mobile clinic.

The Cancer Society’s mobile clinic used by the VSHC team for the outreach clinical work.
Cervical cancer is a preventable cancer, yet it is very common in Fiji. There are more than 100 new cases each year presenting late when a cure is not possible. During this project, 4013 pap smears were conducted and several women were identified with the early stages of the disease when a cure was possible. Follow up of abnormal Pap smear results was conducted by the team, to ensure adequate treatment.
These last four years have brought me back to where I started. Empowerment of women is crucial not only to better reproductive health but also to gender equality and advancement of the societies. There is a huge amount of work to be done to empower women and these efforts will continue.

Educational outreach activities take place under a shady tree.
From 5 November 2012 to 31 December 2014, the project has provided information and education on reproductive health (RH) rights, gender equity and key issues to girls and women.
- 11 103 individuals had education and information provided in RH.
- 1130 advocates trained via workshops.
- 5622 women and girls were provided with RH clinical services.
- 1557 girls and women counselled on contraceptive use and services were provided to those who required them.
- 5333 had breast examinations performed.
- 4016 Pap smears performed for cervical cancer screening.
- 455 women with complicated gynaecological or other problems were referred to the base hospital or VHSC specialist clinic for further specialist services.
References
- MOH annual report 2013
- Carter K, Cornelius M, et al. www.uq.edu/hishub/docs/DN_12pdf .
- WHO STEPs Chronic Disease Risk Factor Surveillance Fact Sheet; www.who.int/chp/steps .
- Carter K, Cornelius M, et al. www.uq.edu/hishub/docs/DN_12pdf .
- Narsey W: https://narseyonfiji.files. wordpress.com/2012/03/gender-issues-in-employment-underemployment-and-incomes-in-fiji.pdf .
- Fiji Women’s Crisis Centre data Somebody’s life; Everybody’s business” 2013.
- Fiji Women’s Crisis Centre data “Somebody’s life; Everybody’s business” 2013.
- Empowerment of Rural Women & Girls in Reproductive Health; a VSHC publication, www.viseiseihealth.org .